牙周手术治疗
21世纪的牙周手术
牙周治疗的目的是预防疾病,减缓或终止疾病进展,重建受损的牙周膜,维持已取得的疗效。它包括多种治疗方法,如龈下刮治、切龈术、改良Widman翻瓣术以及伴有或不伴有骨修整的全厚瓣或断层瓣术。尽管一些纵向临床研究讨论了各种方法的优缺点,但最好的手术方法是什么仍有争议。
第一篇关于牙周治疗方法比较的报道出现于30年前。在那之前,治疗方法的选择基于经验与推理。Ramfjord试图在前瞻性长期研究的结果上建立科学的牙周治疗原则[10,27,28,50,51,54]。他以先锋的姿态挑战了过去长期被人们认同的一些教条,将新的概念引入了牙周病的临床研究。
Ramfjord建议以附着水平的改变作为评价比较牙周治疗的主要指标[10,27,28,50,51,54]。附着丧失被认为是衡量疾病进展的最好指标,这一点将在本章的后面详细谈到。
, http://www.100md.com
对手术治疗进行比较的纵向研究毫无疑问是牙周病学临床研究的重要部分。它们与临床密切相关,可指导医生的日常工作。从事此类研究的中心有7个:密执根、歌德堡、明尼苏达、华盛顿、奥尔胡斯、图森和内不拉斯加。每一个研究组都作出了特有的贡献,为我们现有的知识奠定了基础,并为将来更复杂的研究提供了依据。
密执根最早比较了洁治和袋消除术[54]。袋消除术是指切龈术和伴有或不伴有骨修整的翻瓣术。后来改良Widman翻瓣术,刮治和根面平整也纳入了比较。最初进行的是组间比较,后来发展成了自身对照,这有利控制许多会影响治疗结果的变量。
密执根研究的另一特点是按照初查时的探诊深度进行数据分层:1~3mm、4~6mm、mm以上。结果按照牙齿类型进行比较:上颌磨牙、下颌磨牙、上颌前磨牙、下颌前磨牙、上颌前牙和下颌前牙。最后对全口或分层后的数据进行分析。不同治疗方法、不同初查探诊深度、不同牙齿类型间只有很细微的差别。尽管这种差异没有临床意义,但此研究揭示了确实存在某种差异。
, 百拇医药
虽然袋消除术最大程度减少了探诊深度,但洁刮治、根面平整和改良Widman翻瓣术能更好的改善附着水平。尽管磨牙的疗效稍差,不同牙齿对治疗还是显示了相似的反应。初查时探诊深度较浅的牙齿由于治疗会丧失少量附着,而初查时探诊深度较深的牙齿则有最大程度的附着获得和探诊深度减少。
歌德堡的研究设计更多样化,因此与密执根得出了稍有不同的结论[29-35,42-44,55,59]。Lindhe和Nyman认为只要取得理想的菌斑控制,晚期牙周炎也是能被治愈的[29]。因此研究没有包括不能保证牙列菌斑控制的患者,并为患者提供了2周一次的专业清洁牙齿。研究早期分组比较了:切龈术,伴有或不伴有骨修整的改良Widman翻瓣术和伴有或不伴有骨修整的根向复位瓣术。所有这些方法均能终止附着丧失,但只有在避免骨切除,软组织缝合后完全覆盖牙槽骨时才能获得最大附着[29,43,44,55]。至今没有证据直接显示菌斑是牙周炎的原因,但这些研究确实表明没有菌斑就没有疾病的进展。
此后,歌德堡又自身对照比较了刮治、根面平整和改良Widman术[33-35]。研究关于附着改变和探诊深度减少的发现与Ramfjord相似。(表1)研究确定了洁刮治、根面平整和改良Widman术的临界探诊深度,深度小于它归为附着获得,大于它归为附着丧失。洁刮治,根面平整的临界探诊深度为2.9mm,改良Widman术的临界探诊深度为4.2mm。这一研究完善了治疗反应与初诊探诊深度有关的理论,显示出:
, http://www.100md.com
(1)反应具有治疗特异性;
(2)可准确预计附着获得的水平。这比那种认为特定分层可出现附着获得或丧失的观点更精确。
表1(点击图片可放大)
明尼苏达的研究主要比较了洁刮治、根面平整和改良Widman术[47-49]。6.5年中没有发现治疗组之间的差异。磨牙和非磨牙的附着水平与牙齿丧失差异也很小。奥尔胡斯比较了根向复位瓣术、改良Widman翻瓣术、刮治和根面平整[11-13],也没有发现差异。上述两地的研究设计良好,证实了密执根和歌德堡的研究结果。
华盛顿研究组严格定义了牙槽骨手术是指恢复正常圆弧形骨外形的手术[45,46]。伴有骨修整的根向复位瓣术较单纯根向复位瓣术减少袋深更明显,但可能有轻微附着丧失。作者认为骨修整术能更有效的减少袋深,控制炎症。
, 百拇医药
图森的研究不同于以往之处在于它是在私人诊所而非医科院校进行的[4,5,26]。Berker比较了洁刮治、根面平整、改良Widman术和严格定义的牙槽骨手术。在研究期间内,各治疗组之间只有很小差异。这证实了医科院校的发现,并表明私人诊所也能取得相似的疗效。
内不拉斯加的研究是最近进行的,具有许多设计特点[1,15-25]。
第一,它包括了牙冠洁治组,由于这不是治疗牙周炎的恰当方法,故该组中许多牙齿不得不被排除。
第二,它使用水平向附着水平分析治疗反应。由于治疗方法不同,解释这些数据显得较复杂,但可看出,骨手术的位点复发率最低。
第三,位点按照术后而非初查探诊深度分层。因此疗效的评价实际上是基于维持期的探诊深度,结果发现复发率随探诊深度增加而增加。
, http://www.100md.com 第四,计算了复发位点的年复发率。刮治、根面平整组最高,改良Widman翻瓣术组与其接近,骨手术组最低。
最后,研究还评价了吸烟对疗效的影响,吸烟者对治疗仍有反应,不过相对较弱,并且吸烟者较非吸烟者复发率更高。
对纵向研究的解释
Wang发现牙周治疗后的患者疾病进展速度为每年0.03mm,Westfelt则报道为0.04mm,Loe报道为0.06mm[36-4,58,60]。以0.06mm为标准,疾病将在5年内发展0.3mm,10年内发展0.6mm。另一方面,未经治疗的患者疾病进展更快。Craft报道为每年0.1mm,Axelsson、Lindhe和Loe都报道为每年0.2mm[2,3,8,36-40]。若以0.2mm为标准,5年后疾病进展为1mm,10年后为2mm。治疗组与未治疗组间的差距5年达到0.7mm,10年达到1.4mm。现有器械是很难可靠检测出治疗组和非治疗组间的细微差别的。比较两种治疗方法的效果时,由于疾病年平均进展只有百分之几个毫米,同样也难以发现。多数纵向研究为期不到5年,更没有超过10年,所以很难发现不同治疗组间客观可能存在的差别。
, http://www.100md.com
Jeffcoat&Reddy认为探诊器械的刻度对了解疾病进展有明显影响[14]。使用刻度为0.1mm的阿拉巴马牙釉骨质界探针发现疾病呈持续进展状态,而使用1mm刻度的手用探针则显示疾病是周期爆发式进展的。所以比较治疗方法疗效的不同需要高精度器械。
分析全口平均指标可以很好显示一种治疗方法在该患者身上的疗效。但它掩盖了某些个别的重要位点的变化。表示频率的数据、复发率、疾病进展速度则可以反映个别位点的特殊情况。因此以患者为单位和以位点为单位得到的数据是不同的,需要对它们都进行分析才能阐明治疗效果。而许多纵向研究忽略了这一点,遗留了很多问题。
Machtei通过9个月的观察发现深袋若未经治疗进展比浅袋迅速[41]。研究包括了12名患者,记录了他们的袋深、牙齿类型和颊舌侧探诊位点。对这些数据进行复杂的分析可深入了解个别位点的疾病进展情况。
使用全口平均指标初步纵向研究显示在手术及非手术洁刮治、根面平整间没有疗效差别。但随着设计的改进和数据分析方法的发展,有可能逐渐显现出治疗方法之间的差别。由于浅袋病损复发少,减少袋深将受到重视。
, http://www.100md.com
纵向研究最初选用平均附着水平作为比较疗效的指标。三十年来,这一指标已经发生改变。今后的研究将包括能显示个别位点病损情况的频率数据,每年或累计复发率将用于比较不同治疗方法,个别位点的疾病进展也将用于进一步分析治疗结果。高精度的测量工具将为牙周探诊提供更好的技术。人们还需要改进能确定疾病进展位点的技术。
尽管已有较多关于牙周治疗的长期研究,但仍有许多东西要研究。研究的最终目的是提供可以终止疾病进程并能长期维持疗效的治疗方法。三十年来的研究已推动了这一目标的实现,但还需要更多研究明确每种治疗方法的特点。在现有数据基础上可较好地对患者作出个体化的诊疗。
牙周手术的适应证
牙周炎时,非手术治疗应先于手术治疗进行。只有当非手术治疗失败时才采用手术治疗。一般来说,洁刮治、根面平整后应评价非手术治疗的效果,然后才考虑使用抗菌药物或抗生素,因为这类药物减轻炎症,可掩盖那些洁刮治、根面平整未能起效的位点。那些对非手术治疗有反应并在维持期保持稳定的位点并不需要完全消除牙周袋。但在进行手术治疗时,则应减少探诊深度以方便维持期治疗和减少疾病复发[1,15-25]。牙周手术治疗的优点列于表2。
, 百拇医药
表2(点击图片可放大)
牙周手术的术前准备包括彻底的检查,诊断和全面评估危险因素。患者至少应有80%的牙面清除了菌斑,并且洁刮治和根面平整后应有足够时间供组织愈合。讨论了手术的风险与好处后,患者应签署知情同意书。必要时可用药抑制焦虑和预防心内膜炎。
术后应向患者说明:
(1)可能出现的不适和并发症;
(2)使用的药物,尤其是麻醉药与抗生素;
(3)避免热烫或刺激性的食物与饮料;
(4)减少吸烟,尤其在组织愈合阶段;
(5)家庭卫生指导;
, http://www.100md.com (6)若出现不良反应或其他问题如何就诊。
术后管理简要列于表3。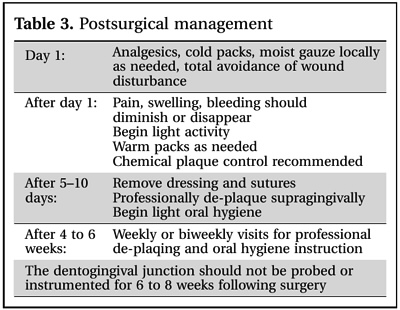
表3(点击图片可放大)
一般牙科医生的角色
一般牙科医生在牙周诊断和治疗中起重要作用。大多数牙周炎都是在普通牙科诊所确诊的。病人是否就诊取决于很多因素,包括病人的愿望和医生提供意见及治疗的倾向。一般牙医通常进行洁刮治和根面平整,外科手术限于探诊深度小于5mm的水平型骨吸收。垂直型骨吸收、Ⅱ度根分叉病变等更严重的病损需要求助于牙周病医生,因为其治疗方法多样并且较困难。第二磨牙远中的楔形瓣术也由于同样原因多由牙周病医生完成。
, http://www.100md.com
手术方法
下面将介绍一般牙科医生适合采用的手术方法:
切龈术(图1.)
该术式用于附着龈足够的情况下去除骨上袋,减轻牙龈增生,或在特定情况下加长牙冠有利美观。一般来说,它不用于:
(1)存在骨内袋时;
(2)需要牙槽骨手术时;
(3)没有足够附着龈时;
(4)系带或肌肉附着造成干扰时;
(5)牙冠太长不利美观时。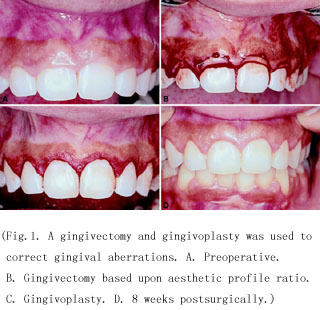
, 百拇医药
图1.切龈术/Gingivectomy(点击图片可放大)
改良Widman翻瓣术(图2.)
Ramforjord & Nissle介绍的这一术式用于去除炎症袋壁,便于根面的清洁并能最大程度保存牙周组织[53]。它尤其适用于需要考虑美观的上颌前牙。其不足之处在于不能消除牙周袋,以长结合上皮形式愈合。
图2.改良Widman翻瓣术/Modified Widman flap
(点击图片可放大)
翻瓣洁治
, 百拇医药
该术式可在直视下清洁根面,减少袋深,并且瓣复位后能最大程度覆盖用于再生的装置。它使用龈沟内切口替代内斜切口。
不进行骨修整的根向复位瓣术
此术式通过根向复位黏膜瓣减少袋深,它为根面预备提供进路,保持或减少附着龈宽度。它使用的是内斜切口。
牙冠延长术(图3.和图4.)
手术延长牙冠:
(1)方便龋坏去除;
(2)为修复提供更多固定位;
(3)建立生物学宽度;
(4)改善美观。
, 百拇医药
只有当余留牙根有健康牙周膜支持并且术后冠根比恰当时才选用此术式。
图3.牙冠延长术/Crown lengthening(点击图片可放大)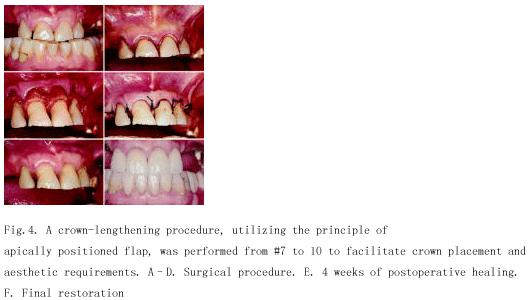
图4.牙冠延长术/Crown lengthening(点击图片可放大)
单个牙侧向转位瓣术
这种手术可覆盖暴露的牙根,防止牙根敏感和根面龋。它用于:
, 百拇医药
(1)孤立的龈退缩;
(2)临近供牙有足够角化牙龈;
(3)前庭沟深度足够。
多个牙有牙龈退缩的区域和供区存在系带附着时不适合采用这种手术。
组织学证明上述翻瓣术以长结合上皮形式愈合,不能形成新的结缔组织附着。但长结合上皮已被证实能维持稳定的疗效[6,7,57,61]。
牙周手术的原则
牙周手术的目的是去除软组织袋壁,感染骨组织,消除牙周袋。目前,手术目标为:
(1)当非手术治疗无效时,为根面预备提供进路;
, 百拇医药
(2)建立合适的牙龈外形;
(3)便于口腔清洁;
(4)延长牙冠便于修复;
(5)通过再生术恢复受损牙周膜。
为确保组织愈合,手术原则应包括:
①充分的麻醉;②表面消毒;③器械锐利;④组织创伤最小化;⑤缩短手术时间;⑥防止不必要的污染;⑦必要时恰当的缝合和塞治。
术后并发症
手术风险包括疼痛、肿胀、出血、药物反应和感染。此外还有牙根敏感、瓣坏死、牙根吸收或固连、牙槽嵴吸收、瓣穿孔、脓肿形成、牙龈外形不规则。Pack & Haber认为并发症的发生率很低(1%)。884例没有使用抗生素的手术只有8例感染,使用抗生素的43例手术只有1例感染。Curtis比较了翻瓣术、骨手术和膜龈手术后出现并发症与疼痛的概率和程度[9]。304例病例中仅5.5%有中到重度疼痛。骨手术引起出血、感染、肿胀或其他不良反应的可能是膜龈手术的3倍。膜龈手术引起疼痛的可能是骨手术的3.5倍,软组织手术的6倍。如果发生术后并发症,应当及时和恰当处理,包括止血、充分镇痛或使用抗生素。
, http://www.100md.com
牙周手术的未来走向
过去牙周治疗仅包括洁刮治、根面平整或切龈术,到今天,它已发展囊括了各种成形和再生术。借助诱导组织再生术,骨和根分叉缺陷已可再生,但还不能完全保证。随着生长因子用于治疗,再生术前景更为广阔,而切除术作为一种牙周治疗方法可能会消失。20年前尚不可能的牙根覆盖现今成为常规手术。新材料的发展消除了使用腭部组织的必要,减少了老年人的牙龈退缩。因此,不久的将来,牙周手术可能会成为牙周治疗的一大特色,其目标是实现组织完全再生。
参考文献
1. Ah MK, Johnson GK, Kaldahl WB, Patil KD, Kalkwarf KL. The effect of smoking on the response to periodontal therapy. J Clin Periodontol 1994: 21: 91-97.
, http://www.100md.com
2. Axelsson P, Lindhe J. Effect of controlled oral hygiene procedures on caries and periodontal disease in adults: results after 6 years. J Clin Periodontol 1981: 8: 239-248.
3. Axelsson P, Lindhe J. The significance of maintenance care in the treatment of periodontal disease. J Clin Periodontol 1981: 8: 281-294.
4. Becker BE, Becker W, Caffesse RG, Kerry GJ, Ochsenbein C, Morrison EC. Three modalities of periodontal therapy. II. 5 year final results. J Dent Res 1990: 69(spec issue): 219.
, 百拇医药
5. Becker W, Becker BE, Ochsenbein C, Kerry G, Caffesse R, Morrison EC, Prichard J. A longitudinal study comparing scaling, osseous surgery and modified Widman procedures. Results after one year. J Periodontol 1988: 59: 351-365.
6. Caton J, Nyman S. Histometric evaluation of periodontal surgery. I. The modified Widman flap procedure. J Clin Periodontol 1980:
7: 212-223. 7. Caton J, Zander HA. Osseous repair of an infrabony pocket without new attachment of connective tissue. J Clin Periodontol 1976: 3: 54-58.
, 百拇医药
8. Craft G. Predicting future bone loss using a new progression rate index for the diagnosis and monitoring of untreated periodontitis. Thesis. Louisville, KY: University of Louisville, 1996.
9. Curtis JW, McLain JB, Hutchinson RA. The incidence and severity of complications and pain following periodontal surgery. J Periodontol 1985: 56: 597-601.
10. Hill RW, Ramfjord SP, Morrison EC, Appleberry EA, Caffesse RG, Kerry GJ, Nissle RR. Four types of periodontal treatment compared over two years. J Periodontol 1981: 52: 655-662.
, 百拇医药
11. Isidor F, Attstr?m R, Karring T. Regeneration of alveolar bone following surgical and nonsurgical periodontal treatment. J Clin Periodontol 1985: 12: 687-696.
12. Isidor F, Karring T. Long term effect of surgical and nonsurgical periodontal treatment. A 5 year clinical study. J Periodontal Res 1986: 21: 462-472.
13. Isidor F, Karring T, Attstr?m R. The effect of root planing as compared to that of surgical treatment. J Clin Periodontol 1984: 11: 669-681.
, 百拇医药
14. Jeffcoat M, Reddy M. Progression of probing attachment loss in adult periodontitis. J Periodontol 1991: 62: 185-189.
15. Kaldahl WB, Johnson GK, Patil KD, Kalkwarf KL. Levels of cigarette consumption and response to periodontal therapy. J Periodontol 1996: 67: 675-681.
16. Kaldahl WB, Kalkwarf KL, Patil KD. A review of longitudinal studies that compared periodontal therapies. J Periodontol 1993: 64: 243-253.
, 百拇医药
17. Kaldahl WB, Kalkwarf KL, Patil KD, Dyer JK, Bates RE Jr. Evaluation of four modalities of periodontal therapy. J Periodontol 1988: 59: 783-793.
18. Kaldahl WB, Kalkwarf KL, Patil KD, Molvar MP. Evaluation of gingival suppuration and supragingival plaque following 4 modalities of periodontal therapy. J Clin Periodontol 1990: 17: 642-649.
19. Kaldahl WB, Kalkwarf KL, Patil KD, Molvar MP. Responses of four tooth and site groupings to periodontal therapy. J Periodontol 1990: 61: 173-179.
, 百拇医药
20. Kaldahl WB, Kalkwarf KL, Patil KD, Molvar MP. Relationship of gingival bleeding, gingival suppuration, and supragingival plaque to attachment loss. J Periodontol 1990: 61: 347-351.
21. Kaldahl WB, Kalkwarf KL, Patil KD, Molvar MP, Dyer JK. Long-term evaluation of periodontal therapy. II. Incidence of sites breaking down. J Periodontol 1996: 67: 103-108.
22. Kaldahl WB, Kalkwarf KL, Patil KD, Molvar MP, Dyer JK. Long-term evaluation of periodontal therapy. I. Response to 4 therapeutic modalities. J Periodontol 1996: 67: 93-102.
, 百拇医药
23. Kalkwarf KL, Kaldahl WB, Patil KD. Evaluation of furcation region response to periodontal therapy. J Periodontol 1988: 59: 794-804.
24. Kalkwarf KL, Kaldahl WB, Patil KD. Patient preference regarding 4 types of periodontal therapy following 3 years of maintenance follow-up. J Clin Periodontol 1992: 19: 788-793.
25. Kalkwarf KL, Kaldahl WB, Patil KD, Molvar MP. Evaluation of gingival bleeding following 4 types of periodontal therapy. J Clin Periodontol 1989: 16: 601-608.
, 百拇医药
26. Kerry G, Becker W, Morrison E, Ochsenbein B, Becker B, Caffesse R. Three modalities of periodontal therapy. I. 5 year final results. J Dent Res 1990: 69(spec issue): 246.
27. Knowles JW, Burgett F, Morrison E, Nissle R, Ramfjord S. Comparison of results following three modalities of periodontal therapy related to tooth type and initial pocket depth. J Clin Periodontol 1980: 7: 32-47.
28. Knowles JW, Burgett FG, Nissle RR, Shick RA, Morrison EC, Ramfjord SP. Results of periodontal treatment related to pocket depth and attachment level. Eight years. J Periodontol 1979: 50: 225-233.
, 百拇医药
29. Lindhe J, Nyman S. The effect of plaque control and surgical pocket elimination on the establishment and maintenance of periodontal health: a longitudinal study in cases of advanced disease. J Clin Periodontol 1975: 2: 67-79.
30. Lindhe J, Nyman S. Alterations of the position of the marginal soft tissue following periodontal surgery. J Clin Periodontol 1980: 7: 525-530.
31. Lindhe J, Nyman S. Long-term maintenance of patients treated for advanced periodontal disease. J Clin Periodontol 1984: 11: 504-514.
, 百拇医药
32. Lindhe J, Socransky S, Nyman S, Westfelt E, Haffajee A. Effect of age on healing following periodontal surgery. J Clin Periodontol 1985: 12: 774-787.
33. Lindhe J, Socransky SS, Nyman S, Haffajee A, Westfelt E. "Critical probing depths" in periodontal therapy. J Clin Periodontol 1982: 9: 323-336.
34. Lindhe J, Westfelt E, Nyman S, Socransky S, Haffajee A. Long term effect of surgical/non-surgical treatment of periodontal disease. J Clin Periodontol 1984: 11: 448-458.
, 百拇医药
35. Lindhe J, Westfelt E, Nyman S, Socransky S, Heijl L, Bratthall G. Healing following surgical/non-surgical treatment of periodontal disease. A clinical study. J Clin Periodontol 1982: 9: 115-128.
36. Loe H, Anerud A, Boysen H. The natural history of periodontal disease in man: prevalence, severity, and extent of gingival recession. J Periodontol 1992: 63: 489-495.
37. Loe H, Anerud A, Boysen H, Morrison E. Natural history of periodontal disease in man. Rapid, moderate and no loss of attachment in Sri Lankan laborers 14 to 46 years of age. J Clin Periodontol 1986: 13: 431-440.
, 百拇医药
38. Loe H, Anerud A, Boysen H, Smith M. The natural history of periodontal disease in man. Study design and baseline data. J Periodontal Res 1978: 13: 550-562.
39. Loe H, Anerud A, Boysen H, Smith M. The natural history of periodontal disease in man. The rate of periodontal destruction before 40 years of age. J Periodontol 1978: 49: 607-620.
40. Loe H, Anerud A, Boysen H, Smith M. The natural history of periodontal disease in man: Tooth mortality rates before 40 years of age. J Periodontal Res 1978: 13: 563-572.
, http://www.100md.com
41. Machtei E, Norderyd J, Koch G, Dunford R, Grossi S, Genco R. The rate of periodontal attachment loss in subjects with established periodontitis. J Periodontol 1993: 64: 713-718.
42. Nyman S, Lindhe J. A longitudinal study of combined periodontal and prosthodontic treatment of patients with advanced periodontal disease. J Periodontol 1979: 50: 163-169.
43. Nyman S, Lindhe J, Rosling B. Periodontal surgery in plaque infected dentitions. J Clin Periodontol 1977: 4: 240-249.
, http://www.100md.com
44. Nyman S, Rosling B, Lindhe J. Effect of professional tooth cleaning on healing after periodontal surgery. J Clin Periodontol 1975: 2: 80-86.
45. Olsen CT, Ammons WF, van Belle G. A longitudinal study comparing apically repositioned flaps with and without osseous surgery. Int J Periodontics Restorative Dent 1985: 5: 10-33.
46. Pack PD, Haber J. The incidence of clinical infection after periodontal surgery. A retrospective study. J Periodontol 1983: 54: 441-443.
, 百拇医药
47. Pihlstrom BL, McHugh RB, Oliphant TH, Ortiz-Campos C. Comparison of surgical and nonsurgical treatment of periodontal disease. A review of current studies and additional results after 61/2 years. J Clin Periodontol 1983: 10: 524-541.
48. Pihlstrom BL, Oliphant TH, McHugh RB. Molar and nonmolar teeth compared over 61/2 years following two methods of periodontal therapy. J Periodontol 1984: 55: 499-504.
49. Pihlstrom BL, Ortiz-Campos C, McHugh RB. A randomized four year study of periodontal therapy. J Periodontol 1981: 52: 227-242.
, http://www.100md.com
50. Ramfjord SP, Knowles JW, Nissle RR, Burgett FG, Shick RA. Results following three modalities of periodontal therapy. J Periodontol 1975: 46: 522-526.
51. Ramfjord SP, Knowles JW, Nissle RR, Shick RA, Burgett FG. Longitudinal study of periodontal therapy. J Periodontol 1973: 44: 66-77.
52. Ramfjord SP, Morrison EC, Burgett FG, Nissle RR, Shick RA, Zann GJ, Knowles JW. Oral hygiene and maintenance of periodontal support. J Periodontol 1982: 53: 26-30.
, http://www.100md.com
53. Ramfjord SP, Nissle RR. The modified Widman flap. J Periodontol 1974: 45: 601-607.
54. Ramfjord SP, Nissle RR, Shick RA, Cooper H Jr. Subgingival curettage versus surgical elimination of periodontal pockets. J Periodontol 1968: 39: 167-175.
55. Rosling B, Nyman S, Lindhe J, Jern B. The healing potential of the periodontal tissues following different techniques of periodontal surgery in plaque-free dentitions. A 2-year clinical study. J Clin Periodontol 1976: 3: 233-250.
, http://www.100md.com
56. Smith DH, Ammons WF Jr, Van Belle G. A longitudinal study of periodontal status comparing osseous recontouring with flap curettage. I. Results after 6 months. J Periodontol 1980: 51: 367-375.
57. Steiner SS, Crigger M, Egelberg J. Connective tissue regeneration to periodontally diseased teeth. II. Histologic observations of cases following replaced flap surgery. J Periodontal Res 1981: 16: 109-116.
58. Wang A. Predicting future bone loss using a new progression rate index for the diagnosis and monitoring of treated periodontitis. Thesis. Louisville, KY: University of Louisville, 1996: 140.
, 百拇医药
59. Westfelt E, Nyman S, Socransky S, Lindhe J. Significance of frequency of professional toothcleaning for healing following periodontal surgery. J Clin Periodontol 1983: 10:148-156
60. Westfelt E, Nyman S, Socransky S, Lindhe J. Significance of frequency of professional tooth cleaning for healing following periodontal surgery. J Clin Periodontol 1983: 10: 148-156.
61. Yukna RA. A clinical and histologic study of healing following the excisional new attachment procedure in rhesus monkeys. J Periodontol 1976: 47: 701-709
责任编辑:王薇, http://www.100md.com
牙周治疗的目的是预防疾病,减缓或终止疾病进展,重建受损的牙周膜,维持已取得的疗效。它包括多种治疗方法,如龈下刮治、切龈术、改良Widman翻瓣术以及伴有或不伴有骨修整的全厚瓣或断层瓣术。尽管一些纵向临床研究讨论了各种方法的优缺点,但最好的手术方法是什么仍有争议。
第一篇关于牙周治疗方法比较的报道出现于30年前。在那之前,治疗方法的选择基于经验与推理。Ramfjord试图在前瞻性长期研究的结果上建立科学的牙周治疗原则[10,27,28,50,51,54]。他以先锋的姿态挑战了过去长期被人们认同的一些教条,将新的概念引入了牙周病的临床研究。
Ramfjord建议以附着水平的改变作为评价比较牙周治疗的主要指标[10,27,28,50,51,54]。附着丧失被认为是衡量疾病进展的最好指标,这一点将在本章的后面详细谈到。
, http://www.100md.com
对手术治疗进行比较的纵向研究毫无疑问是牙周病学临床研究的重要部分。它们与临床密切相关,可指导医生的日常工作。从事此类研究的中心有7个:密执根、歌德堡、明尼苏达、华盛顿、奥尔胡斯、图森和内不拉斯加。每一个研究组都作出了特有的贡献,为我们现有的知识奠定了基础,并为将来更复杂的研究提供了依据。
密执根最早比较了洁治和袋消除术[54]。袋消除术是指切龈术和伴有或不伴有骨修整的翻瓣术。后来改良Widman翻瓣术,刮治和根面平整也纳入了比较。最初进行的是组间比较,后来发展成了自身对照,这有利控制许多会影响治疗结果的变量。
密执根研究的另一特点是按照初查时的探诊深度进行数据分层:1~3mm、4~6mm、mm以上。结果按照牙齿类型进行比较:上颌磨牙、下颌磨牙、上颌前磨牙、下颌前磨牙、上颌前牙和下颌前牙。最后对全口或分层后的数据进行分析。不同治疗方法、不同初查探诊深度、不同牙齿类型间只有很细微的差别。尽管这种差异没有临床意义,但此研究揭示了确实存在某种差异。
, 百拇医药
虽然袋消除术最大程度减少了探诊深度,但洁刮治、根面平整和改良Widman翻瓣术能更好的改善附着水平。尽管磨牙的疗效稍差,不同牙齿对治疗还是显示了相似的反应。初查时探诊深度较浅的牙齿由于治疗会丧失少量附着,而初查时探诊深度较深的牙齿则有最大程度的附着获得和探诊深度减少。
歌德堡的研究设计更多样化,因此与密执根得出了稍有不同的结论[29-35,42-44,55,59]。Lindhe和Nyman认为只要取得理想的菌斑控制,晚期牙周炎也是能被治愈的[29]。因此研究没有包括不能保证牙列菌斑控制的患者,并为患者提供了2周一次的专业清洁牙齿。研究早期分组比较了:切龈术,伴有或不伴有骨修整的改良Widman翻瓣术和伴有或不伴有骨修整的根向复位瓣术。所有这些方法均能终止附着丧失,但只有在避免骨切除,软组织缝合后完全覆盖牙槽骨时才能获得最大附着[29,43,44,55]。至今没有证据直接显示菌斑是牙周炎的原因,但这些研究确实表明没有菌斑就没有疾病的进展。
此后,歌德堡又自身对照比较了刮治、根面平整和改良Widman术[33-35]。研究关于附着改变和探诊深度减少的发现与Ramfjord相似。(表1)研究确定了洁刮治、根面平整和改良Widman术的临界探诊深度,深度小于它归为附着获得,大于它归为附着丧失。洁刮治,根面平整的临界探诊深度为2.9mm,改良Widman术的临界探诊深度为4.2mm。这一研究完善了治疗反应与初诊探诊深度有关的理论,显示出:
, http://www.100md.com
(1)反应具有治疗特异性;
(2)可准确预计附着获得的水平。这比那种认为特定分层可出现附着获得或丧失的观点更精确。
表1(点击图片可放大)
明尼苏达的研究主要比较了洁刮治、根面平整和改良Widman术[47-49]。6.5年中没有发现治疗组之间的差异。磨牙和非磨牙的附着水平与牙齿丧失差异也很小。奥尔胡斯比较了根向复位瓣术、改良Widman翻瓣术、刮治和根面平整[11-13],也没有发现差异。上述两地的研究设计良好,证实了密执根和歌德堡的研究结果。
华盛顿研究组严格定义了牙槽骨手术是指恢复正常圆弧形骨外形的手术[45,46]。伴有骨修整的根向复位瓣术较单纯根向复位瓣术减少袋深更明显,但可能有轻微附着丧失。作者认为骨修整术能更有效的减少袋深,控制炎症。
, 百拇医药
图森的研究不同于以往之处在于它是在私人诊所而非医科院校进行的[4,5,26]。Berker比较了洁刮治、根面平整、改良Widman术和严格定义的牙槽骨手术。在研究期间内,各治疗组之间只有很小差异。这证实了医科院校的发现,并表明私人诊所也能取得相似的疗效。
内不拉斯加的研究是最近进行的,具有许多设计特点[1,15-25]。
第一,它包括了牙冠洁治组,由于这不是治疗牙周炎的恰当方法,故该组中许多牙齿不得不被排除。
第二,它使用水平向附着水平分析治疗反应。由于治疗方法不同,解释这些数据显得较复杂,但可看出,骨手术的位点复发率最低。
第三,位点按照术后而非初查探诊深度分层。因此疗效的评价实际上是基于维持期的探诊深度,结果发现复发率随探诊深度增加而增加。
, http://www.100md.com 第四,计算了复发位点的年复发率。刮治、根面平整组最高,改良Widman翻瓣术组与其接近,骨手术组最低。
最后,研究还评价了吸烟对疗效的影响,吸烟者对治疗仍有反应,不过相对较弱,并且吸烟者较非吸烟者复发率更高。
对纵向研究的解释
Wang发现牙周治疗后的患者疾病进展速度为每年0.03mm,Westfelt则报道为0.04mm,Loe报道为0.06mm[36-4,58,60]。以0.06mm为标准,疾病将在5年内发展0.3mm,10年内发展0.6mm。另一方面,未经治疗的患者疾病进展更快。Craft报道为每年0.1mm,Axelsson、Lindhe和Loe都报道为每年0.2mm[2,3,8,36-40]。若以0.2mm为标准,5年后疾病进展为1mm,10年后为2mm。治疗组与未治疗组间的差距5年达到0.7mm,10年达到1.4mm。现有器械是很难可靠检测出治疗组和非治疗组间的细微差别的。比较两种治疗方法的效果时,由于疾病年平均进展只有百分之几个毫米,同样也难以发现。多数纵向研究为期不到5年,更没有超过10年,所以很难发现不同治疗组间客观可能存在的差别。
, http://www.100md.com
Jeffcoat&Reddy认为探诊器械的刻度对了解疾病进展有明显影响[14]。使用刻度为0.1mm的阿拉巴马牙釉骨质界探针发现疾病呈持续进展状态,而使用1mm刻度的手用探针则显示疾病是周期爆发式进展的。所以比较治疗方法疗效的不同需要高精度器械。
分析全口平均指标可以很好显示一种治疗方法在该患者身上的疗效。但它掩盖了某些个别的重要位点的变化。表示频率的数据、复发率、疾病进展速度则可以反映个别位点的特殊情况。因此以患者为单位和以位点为单位得到的数据是不同的,需要对它们都进行分析才能阐明治疗效果。而许多纵向研究忽略了这一点,遗留了很多问题。
Machtei通过9个月的观察发现深袋若未经治疗进展比浅袋迅速[41]。研究包括了12名患者,记录了他们的袋深、牙齿类型和颊舌侧探诊位点。对这些数据进行复杂的分析可深入了解个别位点的疾病进展情况。
使用全口平均指标初步纵向研究显示在手术及非手术洁刮治、根面平整间没有疗效差别。但随着设计的改进和数据分析方法的发展,有可能逐渐显现出治疗方法之间的差别。由于浅袋病损复发少,减少袋深将受到重视。
, http://www.100md.com
纵向研究最初选用平均附着水平作为比较疗效的指标。三十年来,这一指标已经发生改变。今后的研究将包括能显示个别位点病损情况的频率数据,每年或累计复发率将用于比较不同治疗方法,个别位点的疾病进展也将用于进一步分析治疗结果。高精度的测量工具将为牙周探诊提供更好的技术。人们还需要改进能确定疾病进展位点的技术。
尽管已有较多关于牙周治疗的长期研究,但仍有许多东西要研究。研究的最终目的是提供可以终止疾病进程并能长期维持疗效的治疗方法。三十年来的研究已推动了这一目标的实现,但还需要更多研究明确每种治疗方法的特点。在现有数据基础上可较好地对患者作出个体化的诊疗。
牙周手术的适应证
牙周炎时,非手术治疗应先于手术治疗进行。只有当非手术治疗失败时才采用手术治疗。一般来说,洁刮治、根面平整后应评价非手术治疗的效果,然后才考虑使用抗菌药物或抗生素,因为这类药物减轻炎症,可掩盖那些洁刮治、根面平整未能起效的位点。那些对非手术治疗有反应并在维持期保持稳定的位点并不需要完全消除牙周袋。但在进行手术治疗时,则应减少探诊深度以方便维持期治疗和减少疾病复发[1,15-25]。牙周手术治疗的优点列于表2。
, 百拇医药
表2(点击图片可放大)
牙周手术的术前准备包括彻底的检查,诊断和全面评估危险因素。患者至少应有80%的牙面清除了菌斑,并且洁刮治和根面平整后应有足够时间供组织愈合。讨论了手术的风险与好处后,患者应签署知情同意书。必要时可用药抑制焦虑和预防心内膜炎。
术后应向患者说明:
(1)可能出现的不适和并发症;
(2)使用的药物,尤其是麻醉药与抗生素;
(3)避免热烫或刺激性的食物与饮料;
(4)减少吸烟,尤其在组织愈合阶段;
(5)家庭卫生指导;
, http://www.100md.com (6)若出现不良反应或其他问题如何就诊。
术后管理简要列于表3。
表3(点击图片可放大)
一般牙科医生的角色
一般牙科医生在牙周诊断和治疗中起重要作用。大多数牙周炎都是在普通牙科诊所确诊的。病人是否就诊取决于很多因素,包括病人的愿望和医生提供意见及治疗的倾向。一般牙医通常进行洁刮治和根面平整,外科手术限于探诊深度小于5mm的水平型骨吸收。垂直型骨吸收、Ⅱ度根分叉病变等更严重的病损需要求助于牙周病医生,因为其治疗方法多样并且较困难。第二磨牙远中的楔形瓣术也由于同样原因多由牙周病医生完成。
, http://www.100md.com
手术方法
下面将介绍一般牙科医生适合采用的手术方法:
切龈术(图1.)
该术式用于附着龈足够的情况下去除骨上袋,减轻牙龈增生,或在特定情况下加长牙冠有利美观。一般来说,它不用于:
(1)存在骨内袋时;
(2)需要牙槽骨手术时;
(3)没有足够附着龈时;
(4)系带或肌肉附着造成干扰时;
(5)牙冠太长不利美观时。
, 百拇医药
图1.切龈术/Gingivectomy(点击图片可放大)
改良Widman翻瓣术(图2.)
Ramforjord & Nissle介绍的这一术式用于去除炎症袋壁,便于根面的清洁并能最大程度保存牙周组织[53]。它尤其适用于需要考虑美观的上颌前牙。其不足之处在于不能消除牙周袋,以长结合上皮形式愈合。
图2.改良Widman翻瓣术/Modified Widman flap
(点击图片可放大)
翻瓣洁治
, 百拇医药
该术式可在直视下清洁根面,减少袋深,并且瓣复位后能最大程度覆盖用于再生的装置。它使用龈沟内切口替代内斜切口。
不进行骨修整的根向复位瓣术
此术式通过根向复位黏膜瓣减少袋深,它为根面预备提供进路,保持或减少附着龈宽度。它使用的是内斜切口。
牙冠延长术(图3.和图4.)
手术延长牙冠:
(1)方便龋坏去除;
(2)为修复提供更多固定位;
(3)建立生物学宽度;
(4)改善美观。
, 百拇医药
只有当余留牙根有健康牙周膜支持并且术后冠根比恰当时才选用此术式。
图3.牙冠延长术/Crown lengthening(点击图片可放大)
图4.牙冠延长术/Crown lengthening(点击图片可放大)
单个牙侧向转位瓣术
这种手术可覆盖暴露的牙根,防止牙根敏感和根面龋。它用于:
, 百拇医药
(1)孤立的龈退缩;
(2)临近供牙有足够角化牙龈;
(3)前庭沟深度足够。
多个牙有牙龈退缩的区域和供区存在系带附着时不适合采用这种手术。
组织学证明上述翻瓣术以长结合上皮形式愈合,不能形成新的结缔组织附着。但长结合上皮已被证实能维持稳定的疗效[6,7,57,61]。
牙周手术的原则
牙周手术的目的是去除软组织袋壁,感染骨组织,消除牙周袋。目前,手术目标为:
(1)当非手术治疗无效时,为根面预备提供进路;
, 百拇医药
(2)建立合适的牙龈外形;
(3)便于口腔清洁;
(4)延长牙冠便于修复;
(5)通过再生术恢复受损牙周膜。
为确保组织愈合,手术原则应包括:
①充分的麻醉;②表面消毒;③器械锐利;④组织创伤最小化;⑤缩短手术时间;⑥防止不必要的污染;⑦必要时恰当的缝合和塞治。
术后并发症
手术风险包括疼痛、肿胀、出血、药物反应和感染。此外还有牙根敏感、瓣坏死、牙根吸收或固连、牙槽嵴吸收、瓣穿孔、脓肿形成、牙龈外形不规则。Pack & Haber认为并发症的发生率很低(1%)。884例没有使用抗生素的手术只有8例感染,使用抗生素的43例手术只有1例感染。Curtis比较了翻瓣术、骨手术和膜龈手术后出现并发症与疼痛的概率和程度[9]。304例病例中仅5.5%有中到重度疼痛。骨手术引起出血、感染、肿胀或其他不良反应的可能是膜龈手术的3倍。膜龈手术引起疼痛的可能是骨手术的3.5倍,软组织手术的6倍。如果发生术后并发症,应当及时和恰当处理,包括止血、充分镇痛或使用抗生素。
, http://www.100md.com
牙周手术的未来走向
过去牙周治疗仅包括洁刮治、根面平整或切龈术,到今天,它已发展囊括了各种成形和再生术。借助诱导组织再生术,骨和根分叉缺陷已可再生,但还不能完全保证。随着生长因子用于治疗,再生术前景更为广阔,而切除术作为一种牙周治疗方法可能会消失。20年前尚不可能的牙根覆盖现今成为常规手术。新材料的发展消除了使用腭部组织的必要,减少了老年人的牙龈退缩。因此,不久的将来,牙周手术可能会成为牙周治疗的一大特色,其目标是实现组织完全再生。
参考文献
1. Ah MK, Johnson GK, Kaldahl WB, Patil KD, Kalkwarf KL. The effect of smoking on the response to periodontal therapy. J Clin Periodontol 1994: 21: 91-97.
, http://www.100md.com
2. Axelsson P, Lindhe J. Effect of controlled oral hygiene procedures on caries and periodontal disease in adults: results after 6 years. J Clin Periodontol 1981: 8: 239-248.
3. Axelsson P, Lindhe J. The significance of maintenance care in the treatment of periodontal disease. J Clin Periodontol 1981: 8: 281-294.
4. Becker BE, Becker W, Caffesse RG, Kerry GJ, Ochsenbein C, Morrison EC. Three modalities of periodontal therapy. II. 5 year final results. J Dent Res 1990: 69(spec issue): 219.
, 百拇医药
5. Becker W, Becker BE, Ochsenbein C, Kerry G, Caffesse R, Morrison EC, Prichard J. A longitudinal study comparing scaling, osseous surgery and modified Widman procedures. Results after one year. J Periodontol 1988: 59: 351-365.
6. Caton J, Nyman S. Histometric evaluation of periodontal surgery. I. The modified Widman flap procedure. J Clin Periodontol 1980:
7: 212-223. 7. Caton J, Zander HA. Osseous repair of an infrabony pocket without new attachment of connective tissue. J Clin Periodontol 1976: 3: 54-58.
, 百拇医药
8. Craft G. Predicting future bone loss using a new progression rate index for the diagnosis and monitoring of untreated periodontitis. Thesis. Louisville, KY: University of Louisville, 1996.
9. Curtis JW, McLain JB, Hutchinson RA. The incidence and severity of complications and pain following periodontal surgery. J Periodontol 1985: 56: 597-601.
10. Hill RW, Ramfjord SP, Morrison EC, Appleberry EA, Caffesse RG, Kerry GJ, Nissle RR. Four types of periodontal treatment compared over two years. J Periodontol 1981: 52: 655-662.
, 百拇医药
11. Isidor F, Attstr?m R, Karring T. Regeneration of alveolar bone following surgical and nonsurgical periodontal treatment. J Clin Periodontol 1985: 12: 687-696.
12. Isidor F, Karring T. Long term effect of surgical and nonsurgical periodontal treatment. A 5 year clinical study. J Periodontal Res 1986: 21: 462-472.
13. Isidor F, Karring T, Attstr?m R. The effect of root planing as compared to that of surgical treatment. J Clin Periodontol 1984: 11: 669-681.
, 百拇医药
14. Jeffcoat M, Reddy M. Progression of probing attachment loss in adult periodontitis. J Periodontol 1991: 62: 185-189.
15. Kaldahl WB, Johnson GK, Patil KD, Kalkwarf KL. Levels of cigarette consumption and response to periodontal therapy. J Periodontol 1996: 67: 675-681.
16. Kaldahl WB, Kalkwarf KL, Patil KD. A review of longitudinal studies that compared periodontal therapies. J Periodontol 1993: 64: 243-253.
, 百拇医药
17. Kaldahl WB, Kalkwarf KL, Patil KD, Dyer JK, Bates RE Jr. Evaluation of four modalities of periodontal therapy. J Periodontol 1988: 59: 783-793.
18. Kaldahl WB, Kalkwarf KL, Patil KD, Molvar MP. Evaluation of gingival suppuration and supragingival plaque following 4 modalities of periodontal therapy. J Clin Periodontol 1990: 17: 642-649.
19. Kaldahl WB, Kalkwarf KL, Patil KD, Molvar MP. Responses of four tooth and site groupings to periodontal therapy. J Periodontol 1990: 61: 173-179.
, 百拇医药
20. Kaldahl WB, Kalkwarf KL, Patil KD, Molvar MP. Relationship of gingival bleeding, gingival suppuration, and supragingival plaque to attachment loss. J Periodontol 1990: 61: 347-351.
21. Kaldahl WB, Kalkwarf KL, Patil KD, Molvar MP, Dyer JK. Long-term evaluation of periodontal therapy. II. Incidence of sites breaking down. J Periodontol 1996: 67: 103-108.
22. Kaldahl WB, Kalkwarf KL, Patil KD, Molvar MP, Dyer JK. Long-term evaluation of periodontal therapy. I. Response to 4 therapeutic modalities. J Periodontol 1996: 67: 93-102.
, 百拇医药
23. Kalkwarf KL, Kaldahl WB, Patil KD. Evaluation of furcation region response to periodontal therapy. J Periodontol 1988: 59: 794-804.
24. Kalkwarf KL, Kaldahl WB, Patil KD. Patient preference regarding 4 types of periodontal therapy following 3 years of maintenance follow-up. J Clin Periodontol 1992: 19: 788-793.
25. Kalkwarf KL, Kaldahl WB, Patil KD, Molvar MP. Evaluation of gingival bleeding following 4 types of periodontal therapy. J Clin Periodontol 1989: 16: 601-608.
, 百拇医药
26. Kerry G, Becker W, Morrison E, Ochsenbein B, Becker B, Caffesse R. Three modalities of periodontal therapy. I. 5 year final results. J Dent Res 1990: 69(spec issue): 246.
27. Knowles JW, Burgett F, Morrison E, Nissle R, Ramfjord S. Comparison of results following three modalities of periodontal therapy related to tooth type and initial pocket depth. J Clin Periodontol 1980: 7: 32-47.
28. Knowles JW, Burgett FG, Nissle RR, Shick RA, Morrison EC, Ramfjord SP. Results of periodontal treatment related to pocket depth and attachment level. Eight years. J Periodontol 1979: 50: 225-233.
, 百拇医药
29. Lindhe J, Nyman S. The effect of plaque control and surgical pocket elimination on the establishment and maintenance of periodontal health: a longitudinal study in cases of advanced disease. J Clin Periodontol 1975: 2: 67-79.
30. Lindhe J, Nyman S. Alterations of the position of the marginal soft tissue following periodontal surgery. J Clin Periodontol 1980: 7: 525-530.
31. Lindhe J, Nyman S. Long-term maintenance of patients treated for advanced periodontal disease. J Clin Periodontol 1984: 11: 504-514.
, 百拇医药
32. Lindhe J, Socransky S, Nyman S, Westfelt E, Haffajee A. Effect of age on healing following periodontal surgery. J Clin Periodontol 1985: 12: 774-787.
33. Lindhe J, Socransky SS, Nyman S, Haffajee A, Westfelt E. "Critical probing depths" in periodontal therapy. J Clin Periodontol 1982: 9: 323-336.
34. Lindhe J, Westfelt E, Nyman S, Socransky S, Haffajee A. Long term effect of surgical/non-surgical treatment of periodontal disease. J Clin Periodontol 1984: 11: 448-458.
, 百拇医药
35. Lindhe J, Westfelt E, Nyman S, Socransky S, Heijl L, Bratthall G. Healing following surgical/non-surgical treatment of periodontal disease. A clinical study. J Clin Periodontol 1982: 9: 115-128.
36. Loe H, Anerud A, Boysen H. The natural history of periodontal disease in man: prevalence, severity, and extent of gingival recession. J Periodontol 1992: 63: 489-495.
37. Loe H, Anerud A, Boysen H, Morrison E. Natural history of periodontal disease in man. Rapid, moderate and no loss of attachment in Sri Lankan laborers 14 to 46 years of age. J Clin Periodontol 1986: 13: 431-440.
, 百拇医药
38. Loe H, Anerud A, Boysen H, Smith M. The natural history of periodontal disease in man. Study design and baseline data. J Periodontal Res 1978: 13: 550-562.
39. Loe H, Anerud A, Boysen H, Smith M. The natural history of periodontal disease in man. The rate of periodontal destruction before 40 years of age. J Periodontol 1978: 49: 607-620.
40. Loe H, Anerud A, Boysen H, Smith M. The natural history of periodontal disease in man: Tooth mortality rates before 40 years of age. J Periodontal Res 1978: 13: 563-572.
, http://www.100md.com
41. Machtei E, Norderyd J, Koch G, Dunford R, Grossi S, Genco R. The rate of periodontal attachment loss in subjects with established periodontitis. J Periodontol 1993: 64: 713-718.
42. Nyman S, Lindhe J. A longitudinal study of combined periodontal and prosthodontic treatment of patients with advanced periodontal disease. J Periodontol 1979: 50: 163-169.
43. Nyman S, Lindhe J, Rosling B. Periodontal surgery in plaque infected dentitions. J Clin Periodontol 1977: 4: 240-249.
, http://www.100md.com
44. Nyman S, Rosling B, Lindhe J. Effect of professional tooth cleaning on healing after periodontal surgery. J Clin Periodontol 1975: 2: 80-86.
45. Olsen CT, Ammons WF, van Belle G. A longitudinal study comparing apically repositioned flaps with and without osseous surgery. Int J Periodontics Restorative Dent 1985: 5: 10-33.
46. Pack PD, Haber J. The incidence of clinical infection after periodontal surgery. A retrospective study. J Periodontol 1983: 54: 441-443.
, 百拇医药
47. Pihlstrom BL, McHugh RB, Oliphant TH, Ortiz-Campos C. Comparison of surgical and nonsurgical treatment of periodontal disease. A review of current studies and additional results after 61/2 years. J Clin Periodontol 1983: 10: 524-541.
48. Pihlstrom BL, Oliphant TH, McHugh RB. Molar and nonmolar teeth compared over 61/2 years following two methods of periodontal therapy. J Periodontol 1984: 55: 499-504.
49. Pihlstrom BL, Ortiz-Campos C, McHugh RB. A randomized four year study of periodontal therapy. J Periodontol 1981: 52: 227-242.
, http://www.100md.com
50. Ramfjord SP, Knowles JW, Nissle RR, Burgett FG, Shick RA. Results following three modalities of periodontal therapy. J Periodontol 1975: 46: 522-526.
51. Ramfjord SP, Knowles JW, Nissle RR, Shick RA, Burgett FG. Longitudinal study of periodontal therapy. J Periodontol 1973: 44: 66-77.
52. Ramfjord SP, Morrison EC, Burgett FG, Nissle RR, Shick RA, Zann GJ, Knowles JW. Oral hygiene and maintenance of periodontal support. J Periodontol 1982: 53: 26-30.
, http://www.100md.com
53. Ramfjord SP, Nissle RR. The modified Widman flap. J Periodontol 1974: 45: 601-607.
54. Ramfjord SP, Nissle RR, Shick RA, Cooper H Jr. Subgingival curettage versus surgical elimination of periodontal pockets. J Periodontol 1968: 39: 167-175.
55. Rosling B, Nyman S, Lindhe J, Jern B. The healing potential of the periodontal tissues following different techniques of periodontal surgery in plaque-free dentitions. A 2-year clinical study. J Clin Periodontol 1976: 3: 233-250.
, http://www.100md.com
56. Smith DH, Ammons WF Jr, Van Belle G. A longitudinal study of periodontal status comparing osseous recontouring with flap curettage. I. Results after 6 months. J Periodontol 1980: 51: 367-375.
57. Steiner SS, Crigger M, Egelberg J. Connective tissue regeneration to periodontally diseased teeth. II. Histologic observations of cases following replaced flap surgery. J Periodontal Res 1981: 16: 109-116.
58. Wang A. Predicting future bone loss using a new progression rate index for the diagnosis and monitoring of treated periodontitis. Thesis. Louisville, KY: University of Louisville, 1996: 140.
, 百拇医药
59. Westfelt E, Nyman S, Socransky S, Lindhe J. Significance of frequency of professional toothcleaning for healing following periodontal surgery. J Clin Periodontol 1983: 10:148-156
60. Westfelt E, Nyman S, Socransky S, Lindhe J. Significance of frequency of professional tooth cleaning for healing following periodontal surgery. J Clin Periodontol 1983: 10: 148-156.
61. Yukna RA. A clinical and histologic study of healing following the excisional new attachment procedure in rhesus monkeys. J Periodontol 1976: 47: 701-709
责任编辑:王薇, http://www.100md.com