Colles骨折手法复位小夹板外固定的治疗体会(1)
 |
| 第1页 |
参见附件。
【摘要】目的: 探讨 Colles骨折手法复位及小夹板外固定的方法。方法:自2006年 8月至2009年 12月,本科采用手法复位小夹板外固定治疗 Colles骨折198例。结果:12个月以上随访 180例,均达到临床愈合。复位情况:整复后优 145例,良 32例 ,差 3例,总优良率达 98.3%。6周后掌倾角变小 9例,占 5%。腕关节功能:优138例,良35例,差5例,总优良率达96.1%。结论小夹板具有轻便舒适,固定可靠,调整方便。对于Colles骨折,采用手法复位小夹板外固定,简便易行,经济实用,是一种值得推广的方法。
【关键词】 Colles骨折;手法复位;小夹板外固定
Colles the bone fracture technique repositions outside the small clamping plank the fixed treatment experience
ZhengXinmin
【Abstract】Abstract: Discusses Colles bone fracture technique replacement and outside the small clamping plank the fixed method. Method: From August, 2006 to December, 2009, the undergraduate course uses the technique to reposition outside the small clamping plank to treat the Colles bone fracture 198 examples fixedly. Finally: above 12 months make a follow-up visit 180 examples, achieve the clinical cicatrization. Replacement situation: After the reduction, the superior 145 examples, the good 32 examples, the difference 3 examples, are always fine rate reach 98.3%. 6 weeks later the palm inclination angle changes the small 9 examples, accounts for 5%. Wrist function: The superior 138 examples, the good 35 examples, the difference 5 examples, are always fine rate reach 96.1%. The conclusion small clamping plank has facilely comfortable, fixed reliable, the adjustment is convenient. Regarding the Colles bone fracture, uses the technique to reposition outside the small clamping plank fixed, easy to do, the economy is practical, is method which one kind is worth promoting.
【Key words】 Colles bone fracture; Technique replacement; Outside small clamping plank fixed
【中图分类号】R465【文献标识码】A【文章编号】1005-0515(2011)02-0132-01
Colles骨折即桡骨远端背伸型骨折是急诊科常见伤病,约占平时骨折1/10。多发生于老年妇女、儿童及青年。骨折发生在桡骨远端3cm范围内,多为闭合骨折。一般为间接暴力致伤。跌倒时腕背屈掌心触地,前臂旋前肘屈曲。骨折线多为横形,儿童可为骨骺分离,老年常为粉碎骨折。临床表现为腕部肿胀,疼痛,活动受限。骨折移位明显时,可见餐叉状及枪刺样畸形。笔者回顾性分析了自2006年8月至2009年12月,本科采用手法复位小夹板外固治疗Colles骨折198例,疗效满意,现报告如下。
1 资料与方法
1.1 一般资料:本组病例180例,均为桡骨远端伸直型骨折,其中男53例,女127例;平均年龄11~78岁;稳定性骨折23例,不稳定性骨折157例。致伤原因:摔伤158例,车祸伤17例,坠落伤5例。合并其他部位骨折23例,血气胸3例,腹部闭合性损伤5例。
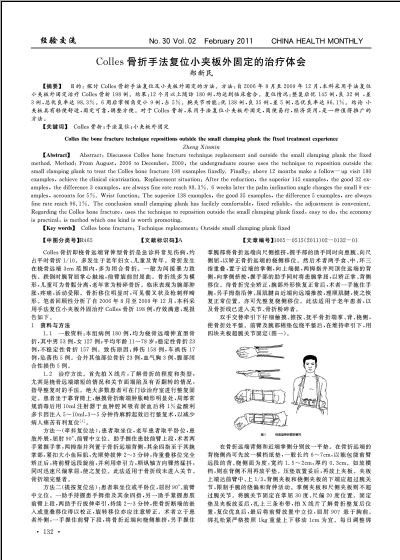
1.2 治疗方法。首先拍X线片,了解骨折的程度和类型,尤其是桡骨远端缩短的情况和关节面塌陷及有否翻转的情况,指导整复时的手法。绝大多数患者可在门诊治疗室进行整复固定。患者坐于靠背椅上,触摸骨折断端肿胀畸形明显处,局部常规消毒后用10ml注射器于血肿腔回吸有淤血后将1%盐酸利多卡因注入5~10ml,3~5分钟待麻醉起效后行整复术,以减少病人痛苦有利复位[1]。
方法一(牵抖复位法):患者取坐位,老年患者取平卧位,患肢外展,屈肘90°、前臂中立位。助手握住患肢前臂上段,术者两手紧握手掌,两拇指并列置于骨折远端背侧,其余四指至于其腕掌部,紧扣大小鱼际肌,先顺势拔伸2~3分钟,待重叠移位完全矫正后,将前臂远段旋前,并利用牵引力,顺纵轴方向骤然猛抖,同时迅速尺偏掌屈,使之复位。此法适用于骨折线未进入关节、骨折端完整者 ......
您现在查看是摘要介绍页,详见PDF附件(2600kb)。